Introduction
In the precedent article, I performed a virtual surgery by adding implants. I redid a virtual surgery keeping the previous implants and adding one on the left side. This is the side where the airflow is most poorly distributed between the middle meatus and the inferior meatus. So I would like to improve that with this new implant.
Virtual implant placement

This cut is made a little after the anterior part, in blue is represented the previous implant, and in red is the one that I have just added. I designed this implant to try to better respect the rule that I had written in the previous article which is to have between 1.5 and 3 mm between the walls everywhere in the nasal cavity. And we can clearly see that this was not the case here.
Results
Streamlines
Before

After

In the area circled in red, we can see an increase in airflow (more streamlines). It's not huge but significant.
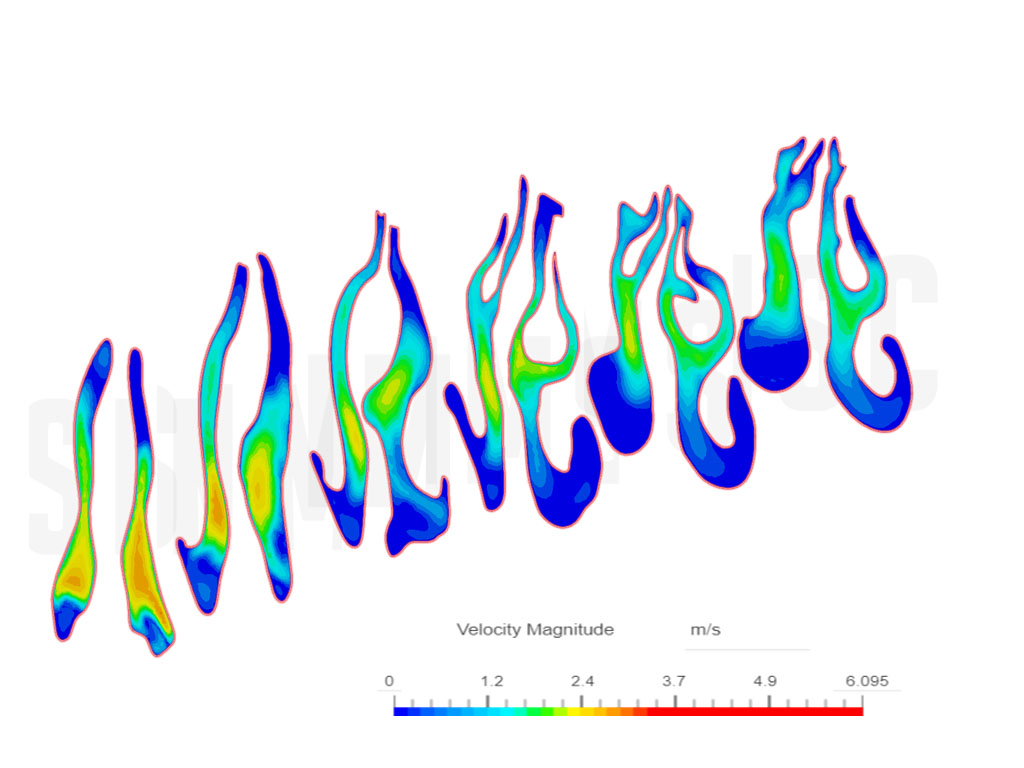
Velocity
Before



After



In the central illustration, we can see that after the virtual implant at the level of the inferior meatus an area changes from light blue to green, but it is quite subtle. It is a very minor change.
Wall Shear Stress
Before



After



We can see that in the first view where the virtual implant is placed there is an increase in WSS (red arrows). It is not surprising because the implant has moved the wall closer to the airflow. On the other hand, it is quite disappointing to see no change in the inferior meatus, the increase in airflow has not translated into an increase in WSS. I think the increase in airflow is not high enough to see a significant change in terms of WSS.
Nasal resistance and airflow symmetry
Discussion
I already talked about it in the previous article, I think it's very important to restore the "ideal" distance (from 1.5 to 4 mm) between the walls. And that's what I tried to do with this new virtual implant. From my point of view, this ideal distance must be restored everywhere in the nasal cavity. I think it's one of the best strategies to improve several key points:
- The distribution of the airflow and the WSS between the middle meatus and the inferior meatus.
- The increase in average WSS.
- The stability of the cross-sectional area.
- The nasal resistance.
This is exactly what the body does after a rapid change in the anatomy of the nasal cavity, for example after a deviation of the septum. Indeed there is a correlation between the deviation of the septum and the formation of a concha bullosa [1]. In this study, the authors say:
"We also found that there was a strong relationship between the presence of a concha (unilateral or a dominant concha) and deviation of the nasal septal convexity away from the concha (P < .0001). We also found, however, that there was always maintenance of the nasal air channel between the medial aspect of the concha (unilateral or dominant concha) and the adjacent surface of the nasal septum"
Examples of concha bullosa


The interpretation that we can have is that the "body" does this in order to restore the ideal distance between the walls. And if he does that, there is surely a certain utility.
Conclusion
Adding this virtual implant did not drastically change the airflow, however, I think this optimization is useful. Note that I have not talked about nasal resistance and airflow symmetry in the article because the change is minor after this virtual implant.
References
- The Incidence of Concha Bullosa and Its Relationship to Nasal Septal Deviation and Paranasal Sinus Disease, Jamie S. Stallman, Joao N. Lobo and Peter M. Som
Introduction
In this article, I will compare many parameters before and after the virtual implants to see if there are improvements. But before I would like to explain the causes of ENS because before finding solutions it is necessary to understand the problem correctly. In the second paragraph, I will define goals. What parameters do I think I can improve with these virtual implants.
In the article I will speak about different regions in the nasal cavity, to be clear here is an illustration.I
n red the anterior part which is the beginning of the nasal cavity, in green the middle meatus, it is where the middle turbinates are and finally in blue the inferior meatus where the inferior turbinates are.

Causes of ENS

The Empty Nose Syndrome can be caused by a partial or a complete cut of the inferior or middle turbinates. It can even be caused by a burn of the mucosa. The cut causes a loss of volume, that's to say an increase in emptiness and a reduction in the mucosa surface. The burn affects negatively the health of the mucosa. All of this has many effects:
- The increase in emptiness causes:
- A modification in the distribution of the airflow, most of the airflow is redirected in the middle meatus in case of an inferior turbinectomy [1].
- An increase in the cross-sectional area which reduces the velocity of the airflow and affects negatively the Wall Shear Stress. Less WSS means less evaporation of the mucus due to the airflow passage which leads to less cooling effect of the mucosa. Indeed the change of the mucus from the liquid state to the gaseous state leads to energy consumption which cools the mucosa. And it is this cooling that detects the TRPM8 receptors and gives us the feeling of the airflow [2]. The increase in the cross-sectional area also reduces nasal resistance.
- The reduction in the mucosa surface causes:
- A reduction in the numbers of TRPM8 receptors simply because the receptors are in the mucosa and the fewer mucosa there are, the fewer receptors there are.
- A reduction of the production of mucus because it is the same thing, the glands that produce mucus are found in the mucosa [3].
- A reduction in the number of blood vessels which can decrease the temperature of the mucosa. Simply because the mucosa is kept at the right temperature thanks to the blood flow.
- The cut of turbinates disturbs the nasal cycle because a large part of the turbinates has disappeared. The nasal cycle is the phenomenon that consists of vasodilation of the turbinates on one side and then the other over a cycle of a few hours. However, it seems that the utility of the nasal cycle is still unknown [4]. But the phenomenon of vasodilatation/vasoconstriction has another very important role which is to adapt the cross-sectional area according to physical activity. Indeed during physical activity the airflow increases, in response to this, the turbinates decrease in volume via the phenomenon of vasoconstriction [5].
Goals of the virtual implants
The thing that seems not possible to do with implants is to increase the mucosa surface, an implant just moves the mucosa. In some cases, it can create a bit of a mucosa surface by stretching it but it can't be a major increase.
What it is possible to do is to decrease the emptiness, so decrease the cross-sectional area. The goal is to design the implants in order to:
- Have a better airflow distribution between the middle and the inferior meatus because it seems that this parameter has a great impact on ENS symptoms [1].
- Have a better repartition of WSS between the two regions and increase it in the region affected by the turbinectomy. Because WSS plays a major role in airflow sensation as I explained in the causes of ENS. In this study [1], the researchers found a correlation between WSS value in the lower meatus and the sensation of suffocation. “Among the 6 items in ENS6Q, complaints of “suffocation” and “nose feels too open” were significantly correlated with peak WSS in the inferior turbinate region”
Interestingly they found no correlation between nasal resistance and ENS symptoms. “Nasal resistance did not correlate with ENS6Q or any other symptom score”.
Virtual implants placement



Virtual implants appear in red, we can say that there are 3 implants in the left nasal cavity, one on the floor, one in the nasal wall, and a small one in the septum. On right it is a pretty big implant, note that I don’t know if this implant is possible to do because it is placed behind my existing implant and the shape that I have designed is huge.
What I tried to do by designing these implants is to restore the "ideal" distance between the walls. Let me explain what I call the “ideal” distance between walls. When we see a healthy nasal cavity CT-SCAN we can see that the distance between two walls is almost the same everywhere. I measured it, it's between 1.5 and 3 mm. So I designed these implants to tend to these values without reaching them everywhere due to technical constraints. I tried to respect what could be done in terms of implantation with a big doubt about the right implant.

Change of the cross-sectional area

After the virtual implant, it is not surprising that the cross-sectional area has decreased and it is a little more regular throughout the nasal cavity.
Note that the values of the control groups are pulled from this study [6], but I measured myself some healthy CT-SCANs and I found values between 250 and 300 mm² of total cross-sectional area instead of the 200mm² in the study. So I don’t know what the normal values are. Maybe it is a range between 200 and 300 mm², I don’t know. The area also depends on body position and physical activity but I assume almost all ct-scans are done while lying down. The values obtained are therefore comparable.
Results
Streamlines
Before virtual implants


In the previous article I had not shown the right side, we can see that there is a bit better distribution of the airflow on this side.
After virtual implants

We can see that there is almost no change in the airflow distribution. Maybe in the left side view, there is a bit more streamlines in the inferior meatus. But it is not a huge improvement.


Velocity
Before virtual implants

After virtual implants

All surfaces that have an airflow velocity greater than 2.5 m/s are in red. The peak is at 3,24 m/s.
Same thing here no real improvement in velocity.
Wall Shear Stress
Before virtual implants

After virtual implants

All the walls that have a greater WSS than 0,1 Pa are in red. The peak is at around 0,9 Pa.
We can see a real change here, in the areas where the virtual implants are placed the walls are more “colored”. Which means that the WSS is higher.


In these cuts, we can clearly see that the virtual implant has increased the WSS. Now there is blue and even yellow color, which means that the WSS has increased from almost 0 Pa to values between 0,025 and 0,07 Pa.


Same thing here, there is more WSS, especially on the right side. What I can say is that it is really a positive change, concretely this improvement of the WSS should improve the feeling of the airflow in the inferior meatus. The virtual implants simply moved the walls closer to the airflow. I think it's a good strategy to adopt, identify the airflow and then bring the walls closer to the airflow in order to increase the WSS while respecting the minimum distance between the walls (1,5 - 3 mm).
Airflow humidity
Before virtual implants

After virtual implants

We can see that there is almost no change in the airflow humidity.
Airflow temperature
Before virtual implants

After virtual implants

There is a little bit less green and yellow in the last slice which means that the airflow temperature is a bit higher after the virtual implants. The temperature in the scalebar is in Kelvin so you need to subtract 273 to obtain the temperature in Celcius. And also you need to multiply by 100 before that. So for example in red the temperature is equal to 3,096*100= 309,6°K and then 309,6 - 273 = 36,6°C.
Nasal resistance and airflow symmetry

If your CFD results are in the green square you have a high probability of having normal nasal resistance and normal airflow symmetry. The resistance R is on the horizontal axis and the airflow symmetry theta (𝚹) is on the vertical axis. You can see how these indicators are calculated in this study here [7].
Airflow symmetry
Before virtual implants, the flow rate is at 7 l/min on the left and 7,3 l/min on right. This corresponds to a 𝚹 of 1,028 which is very good, the flow is almost the same in the right nasal cavity than in the left. After virtual implants, the flow rate is at 6,9 l/min on the left and 7,68 l/min on right. This corresponds to a 𝚹 of 1,097 which is a bit less good but it’s still normal according to Flowgy. So if I wanted to correct this I would have to design a smaller implant on the right or a bigger one on the left.
Nasal resistance
Nasal resistance R is calculated based on several parameters like the difference of pressure between the environment and the pharynx (delta P), the flow rate, the density of air, and the area of the nostrils. When the air passes through the nasal cavity, it undergoes a loss of pressure due to the friction on the walls, it is the delta P.
Before virtual implants, the value is 4,7 and after 6,94, it is not surprising that the value has increased because the virtual implants have decreased the cross-sectional area in certain regions of the nasal cavity.
This is rather a good thing because according to the graph the value was barely within the norm. After the implants, the values have progressed a bit in the right direction. But note that the absolute value of R is not very precise because it depends on a lot of parameters in the simulation. It's just an indicator to see if the virtual surgery has changed the value in the right direction. Also, this value seems to have no impact on the ENS symptoms as I mentioned in the “goals” paragraph. But I still think it's a good thing to be in the norm because nasal resistance is useful for normal lung function [8].
Conclusion
One of the goals was not achieved, the airflow distribution did not improve. I don't really know how to improve it, especially on the left side where it is particularly bad.
However, the virtual implants have greatly improved the WSS which is a positive thing. Also, the airflow temperature and the nasal resistance are a bit higher.
So I think that this kind of implant can be useful, especially for the airflow sensation.
References
- Investigation of the abnormal nasal aerodynamics and trigeminal functions among empty nose syndrome patients, Chengyu Li, PhD, Alexander A. Farag, MD, Guillermo Maza, MD, Sam McGhee, Michael A. Ciccone, Bhakthi Deshpande, MA, Edmund A. Pribitkin, MD, Bradley A. Otto, MD, and Kai Zhao, PhD
- Empty Nose Syndrome Pathophysiology: A Systematic Review, Jeanie Sozansky BS, Steven M. Houser MD,
- Submucosal glands, Wikipedia
- The nasal cycle in health and disease, J. Hanif
- Sataloff's Comprehensive Textbook of Otolaryngology: Head & Neck Surgery, Robert T Sataloff, chapter 19, p 286
- Computational fluid dynamics and trigeminal sensory examinations of empty nose syndrome patients, Chengyu Li , Alexander A Farag , James Leach , Bhakthi Deshpande, Adam Jacobowitz , Kanghyun Kim , Bradley A Otto , Kai Zhao
- Robust nondimensional estimators to assess the nasal airflow in health and disease, E. Sanmiguel-Rojas M. A. Burgos C. del Pino M. A. Sevilla-García F. Esteban-Ortega
- Surgery of the turbinates and “empty nose” syndrome, Marc Oliver Scheithauer, paragraph 8
Introduction
First of all, what is Flowgy? Flowgy is a software dedicated for CFD of the nasal cavity with tools for virtual surgery. In this article, I will compare the results that I got with my industrial software (Onshape and Simscale) and the results with Flowgy. I would like to thank Pr Manuel Burgos for loaning me the software and answering all my questions.


I set the max speed at 3,25 m/s in both software. We can see the same thing, most of the airflow passes through the middle meatus. Note that on Flowgy I just showed the airflow in the left nasal cavity to see more clearly what is going on.
Cuts - Velocity

The main difference in the two views is the max speed, it is set at 3,5 m/s in Simscale and 2,5 m/s in Flowgy because I was not able to set 3,5m/s in Flowgy. But we can roughly see the same thing, the speed of the airflow is very lower in the inferior meatus. It's reassuring to see the same thing because it means that the 3d model I drew of my nasal cavity was quite accurate.
Wall Shear Stress
Now the really interesting thing in Flowgy is that there are other data available, one of them that is particularly interesting in the ENS context is the Wall Shear Stress (WSS). I already mentioned WSS in other articles. I will explain a bit more about what WSS is and why it is particularly interesting data in the ENS context. WSS is the pressure exerted by the airflow to the walls, the unit is the Pascal (Pa). The higher the gradient of velocity near the wall the higher the WSS. It is an important value because it is the WSS that gives the airflow sensation.


The pressure higher than 1 Pa is represented in red. We can see that the max WSS is located mostly in the anterior part and also in the middle meatus which corresponds to the velocity of the airflow. So we want to have a better distribution of the WSS between the middle and inferior meats. This is what I will try to do with virtual implants in the next article.
Airflow humidity

In this view is represented the humidity of the airflow, we can of course see that it increases as it passes through the nasal cavity. We can see that part of the airflow is at 92% humidity in the last cut. The values are certainly not very precise. By default in the simulation parameters, the mucosa is at 100% humidity which is a little optimistic given that we often have the mucosa dry because of the ENS. At the same time, the value of the inspired air is set to 20% humidity which is pessimistic because often the outside air is more humid than this. What will be interesting is the comparison before/after the virtual implants so the input parameters are not so important.
Airflow temperature

Same thing here with the temperature of the airflow, in the simulation parameters the mucosa is set at 309,65°K which is 36,65°C. The inhaled air is set at 21,15°C. The temperature of the mucosa is also maybe a little optimistic in the context of ENS. I think the entrance to the nose is colder than that due to the lack of mucosa. But I can't quantify it and it will depend on the aggressiveness of the turbinectomy. In this illustration, the minimum temperature is set at 300°K (27°C) in blue.
Conclusion, what’s next?
Flowgy gives us really interesting data which will be valuable to compare before and after the addition of virtual implants. I'll talk about it in the next article, but I think it's no longer possible to do nose surgery in 2022 without first having done a virtual surgery to see what it will give in terms of airflow, WSS, etc …
Now I will try to design virtual implants in order to improve airflow distribution, WSS distribution, etc …
Introduction
As planned I designed virtual implants in my nasal cavity in order to improve airflow distribution and decrease cross-sectional area to tend toward a healthy nose.
Virtual implants placement

In red are the virtual implants that I designed, you can see that I added a lateral wall implant behind the existing one on the right side. It measures approximately 30 mm long, 10mm high, and 5mm thick.
On the other side, we can say that it is two implants, a floor, and a lateral wall implant.
The floor implant measures approximately 35 mm long, 6mm wide, and 3 mm thick.
And the lateral wall implant is 35 mm long, 10 mm high, and 2 mm thick.
So I don't know if it is even possible to add an implant behind the existing one but I think that it is a good idea to keep the cross-sectional area constant all along the right side.
On the left side, I added two implants which aim to reduce the space between the existing inferior turbinates and the walls.
Cross-sectional area change
We can see that the change starts at 40 mm from the nostrils until 70 mm. And now we reach a maximum of around 400 mm² instead of 500 mm², but it is still far from a healthy nose. So we can already say that the implants are not big enough. But my first goal was to try to have a better flow distribution and a constant cross-sectional area.
Results


We can quickly see that there is almost no change in the airflow distribution and velocity. There is maybe a bit more airflow in the inferior meatus but it is not a crazy change.
Before virtual implant
After virtual implant

In the slice view If we compare before and after virtual implants, we also do not see any significant difference in airflow velocity.


I made a slice with the same distance from the nostrils of the two 3d models (before and after virtual implants). And I placed a dot to measure the velocity at the same location. After virtual surgery, the velocity is around twice higher 0,26 m/s instead of 0,14 m/s in the post-virtual surgery 3d model. But it is just a little area, we can see the color change and it is twice higher yes but 0,26 m/s is still a very low velocity to the 2 m/s in green for instance. So I speculate that this change is almost not perceptible in terms of airflow feeling.
Conclusion and next step
So what I can say with those data is these virtual implants have almost changed nothing in the velocity and the airflow distribution. It's possible that if these implants were done in reality I would feel almost no improvements. But one thing, ENS symptoms are not just due to airflow problems, there is also the health of the mucosa, the nasal cycle which is almost dead with cutted turbinates and maybe others things to take into account.
What is the next step?
Find better implants placement, also maybe bigger implants to decrease cross-sectional area … I don't know.
Recreate true turbinates… Ok it is not possible in reality.
Introduction
Finally, I was able to make a 3d model of my nasal cavity usable with a CFD software.
For those who don't know what is CFD, it just mean Computational Fluid Dynamics which is the study of fluids, in our case the air.
I took 15 l/min for the flow rate and I did not apply temperature conditions on the walls.
Just for information each nostril has a surface of around 68 mm² and the beguining of my pharynx 420 mm². And you can see my cross-sectional area here, in my precedent article.
Results

In this view, the airflow is represented by tiny tubes. We can see that almost all the airflow passes through the middle meatus at a velocity between 1,5 and 2 m/s. On the opposite in the inferior meatus zone, there is almost no airflow and the velocity is very low, less than 0,5 m/s. Near the nostrils, in some areas, the velocity is pretty high around 3 m/s.

Same thing for the left side.
In this view, the nasal cavity is sliced, at the left of the illustration it is near the nostril, and at the right near the pharynx. We just see the velocity not the quantity of airflow, and we can see the same thing that in the other views, very low velocity in the inferior meatus despite my right nasal wall implant.
Results interpretation
The results are not very surprising, some studies come to the same conclusion about the airflow distribution. In this study for instance they showed the same thing, an important reduction of the airflow in the inferior meatus (25.8% ± 17.6%) . They also showed a reduction in wall shear stress (WSS) in the inferior meatus area, which is the force of friction on the walls of the mucosa. Less shear stress means less airflow sensation. And I'm not sure but less airflow quantity and less velocity mean less wall shear stress. In my simulation, I was not able to measure the wall shear stress due to software limitations but since the velocity and the airflow are very low in the inferior meatus then we can say that the WSS too. And according to this same study, the symptoms "of "suffocation" and "nose feels too open" were also found to be significantly correlated with peak WSS around the inferior turbinate. So in others words less WSS in the inferior meatus zone mean more symptoms of suffocation and the feeling of the nose too open.

Conclusion and next step
Now that we clearly see that one of the problem in ENS is the airflow distribution, I will try to fix that with some virtual implants placed in differents area. The goal of course is to tend towards the same airflow distribution of a heathy nose.
Limitations
Just to be clear, I'm not a reasearcher nor a CFD specialist, so the results can be wrong due to many things. If you see an error in the conditions or the reasoning, please can contact me.