Nasal obstruction and its treatments
Nasal obstruction is caused by turbinates inflammation or other diseases that can swell turbinates or a deviated septum.
Nowadays, the first line of treatment to reduce nasal obstruction is by medication and if that doesn’t help, surgical procedures are considered. Here is a list of the common interventions:
Temporary medical treatments: nasal decongestant, antihistamine, allergy desensitization, nasal expander.
Permanent surgical interventions (from least invasive to most invasive): radiofrequency, septoplasty, bipolar probe, submucosal resection, turbinoplasty, turbinectomy.
The timeline of surgical interventions usually starts with bipolar probe or radiofrequency which are less invasive procedures under local anesthesia that can reduce the size of the turbinate. If these methods prove unsuccessful, other surgical procedures (submucosal resection, turbinoplasty, septoplasty, turbinectomy) are usually proposed. However, they are more invasive and often performed under general anesthesia. All surgical procedures on the turbinates hold a risk of causing ENS.
Let alone the risks of ENS, we know that cutting turbinates even partially is not the solution for nasal obstruction. Indeed the reduction of turbinate volume necessarily negatively affects their functions which are the following: sense of airflow, humidification, and heating of inhaled air, and adaptation of nasal resistance according to oxygen consumption. Burning them with laser or radiofrequency devices destroys the mucosa, and cutting with a scissor destroys everything. Even sub-mucosal reduction can affect nerves and damage the mucosa.
Luckily, another surgical procedure exists that has become increasingly common in recent years: it is called MSE (Maxillary Skeletal Expansion). In essence, this procedure expands the nasal cavity instead of cutting the turbinates. Think “pushing the walls of the room instead of removing the furniture”. We give an overview of this procedure in the present article.
Why do we have small nasal cavities along with underdeveloped jaws and airways?
Before we take a close look at the MSE procedure, let’s take a step back and understand the likely causes of our small nasal cavities.
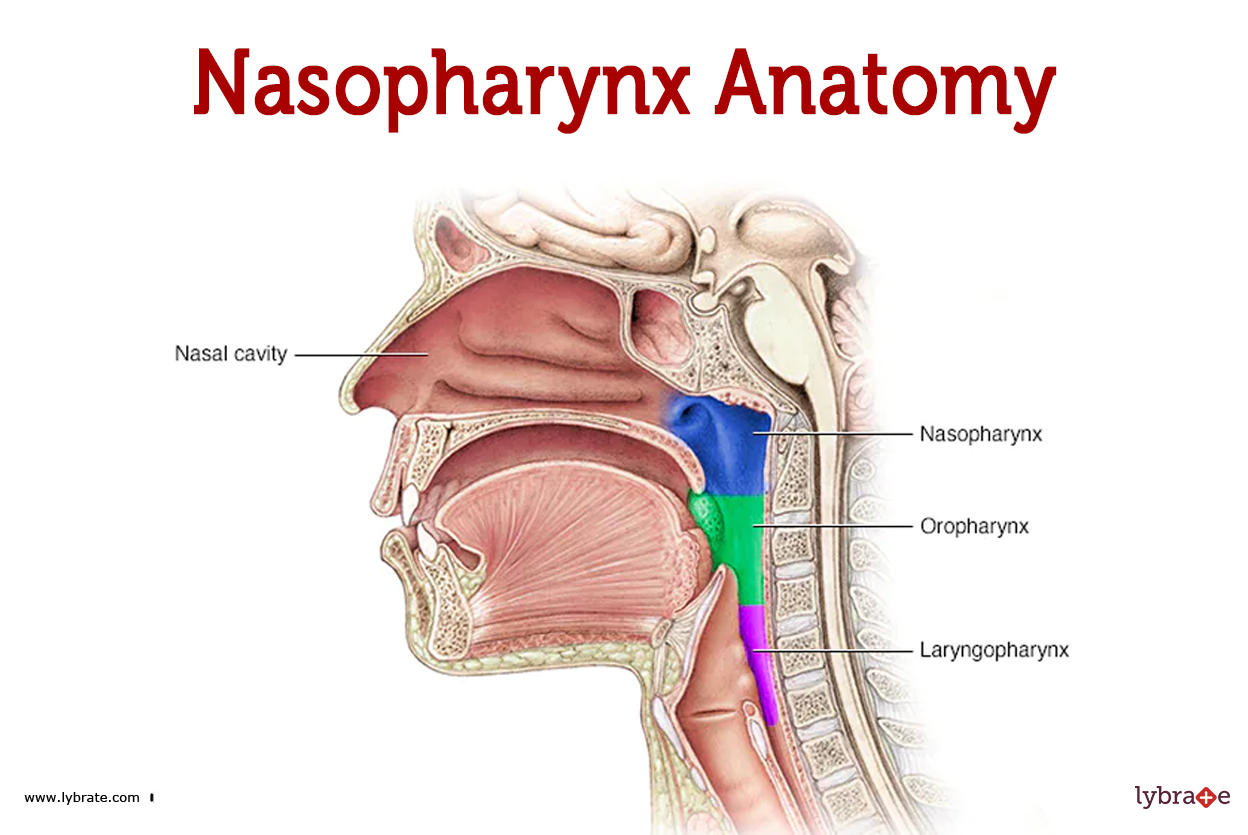
In modern western societies, most of us suffer from craniofacial dystrophy. In a nutshell, this means elongated faces, deviated septums, small nasal cavities, narrow and high-arched palates, crooked teeth, small and recessed jaws… In the throat, the airway is small because our recessed jaws push the tongue backward. This is why sleep apnea is becoming increasingly prevalent.
The main causes of craniofacial dystrophy according to the book Jaws which comprises over 200 scientific references are:
- The food we eat is too calorie dense and way too soft compared to what humanity ate pre agriculture that’s to say more than 10 000 years ago. Our modern food requires too little chewing, and it is chewing that stimulates jaw growth during childhood.
- Mouth breathing impacts jaw development, it lengthens the face and narrow it in the direction of width and depth. Mouth breathing has several causes, allergy, weak jaw muscle due to lack of chewing, common colds…
- Other causes, no breastfeeding or not long enough, bad posture etc ...
For more details about this topic, we invite you to read this article in BioScience and this book.
Why is expanding the maxilla the solution?
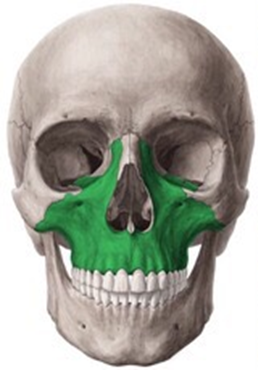
Instead of cutting the lower turbinates to create space in the nasal cavity which disturbs the delicate physiology of the nose, another solution has become increasingly popular in recent years: maxillary expansion. The maxilla is the bone in the middle of the face, and maxillary expansion refers to the expansion of this bone through the palatal suture.
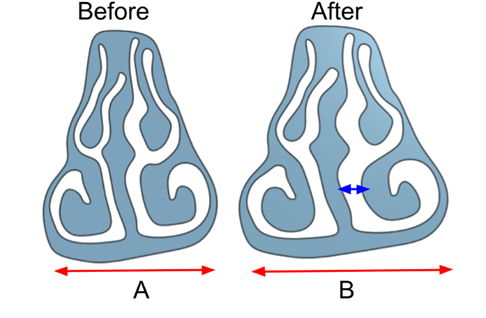
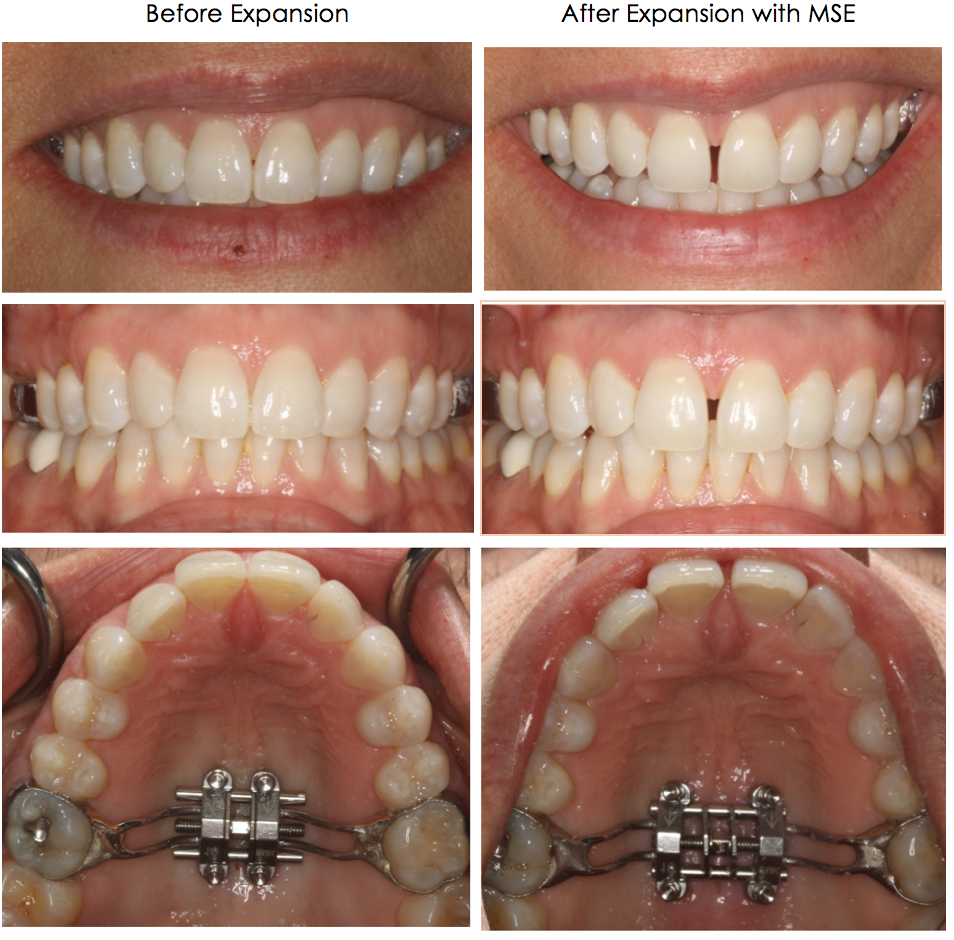
The hard palate which is a part of the maxillary bone serves as the base of the nasal passage. Consequently, by expanding the hard palate, the nasal passage gets wider. A wider nasal passage allows for more air to flow in the nose – no more obstruction! This avoids destroying mucosa with radiofrequency or cutting it off with scissors… In fact, expansion can even create some mucosa on the nasal floor.
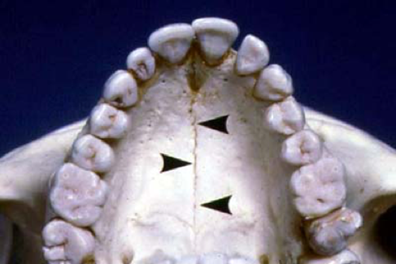
The hard palate presents a suture that starts to fuse around puberty and becomes increasingly tight until about age 25 when it becomes tightly fused and hard to break apart. Therefore, the suture must be surgically cut prior to starting the expansion in adults. While this might sound just as invasive as turbinectomy, it is far from it because the turbinates play an essential role in breathing and nasal physiology, while the palate’s only role is structural – to be the roof of the mouth and the floor of the nasal cavity. With palate expansion, no tissue is cut off with scissors, a cut is made on the suture which can be done under local anesthesia and remains rather painless. Turbinectomy usually requires general anesthesia and multiple days or even weeks without being able to breathe through the nose because of nose plugs and crust build-up. Maxillary expansion on the other hand can require orthodontic treatment because as the palate expands, the teeth separate temporarily creating a diastema. In some cases, the diastema closes by itself without orthodontic treatment, but it depends on the type of expander used.
Methods for expanding the Maxilla
Some orthodontists have tried to split the suture without prior surgical assist, and while this can work on younger patients or on women who have a less tightly fused suture, it comes at the risk of failing to split the suture, pushing teeth out of the alveolar bone and asymmetric expansion. Therefore, in most cases, maxillary expansion takes place with a surgical assist.
Traditionally, expansion was done in conjunction with a Lefort 1 cut which is the cut of the maxillary bone above the roots of the teeth as shown in this slide from Dr Coppelson’s presentation. Please understand the Lefort 1 cut and the palatal suture cut are two different cut. The Lefort 1 is horizontal while the palatal suture is vertical.

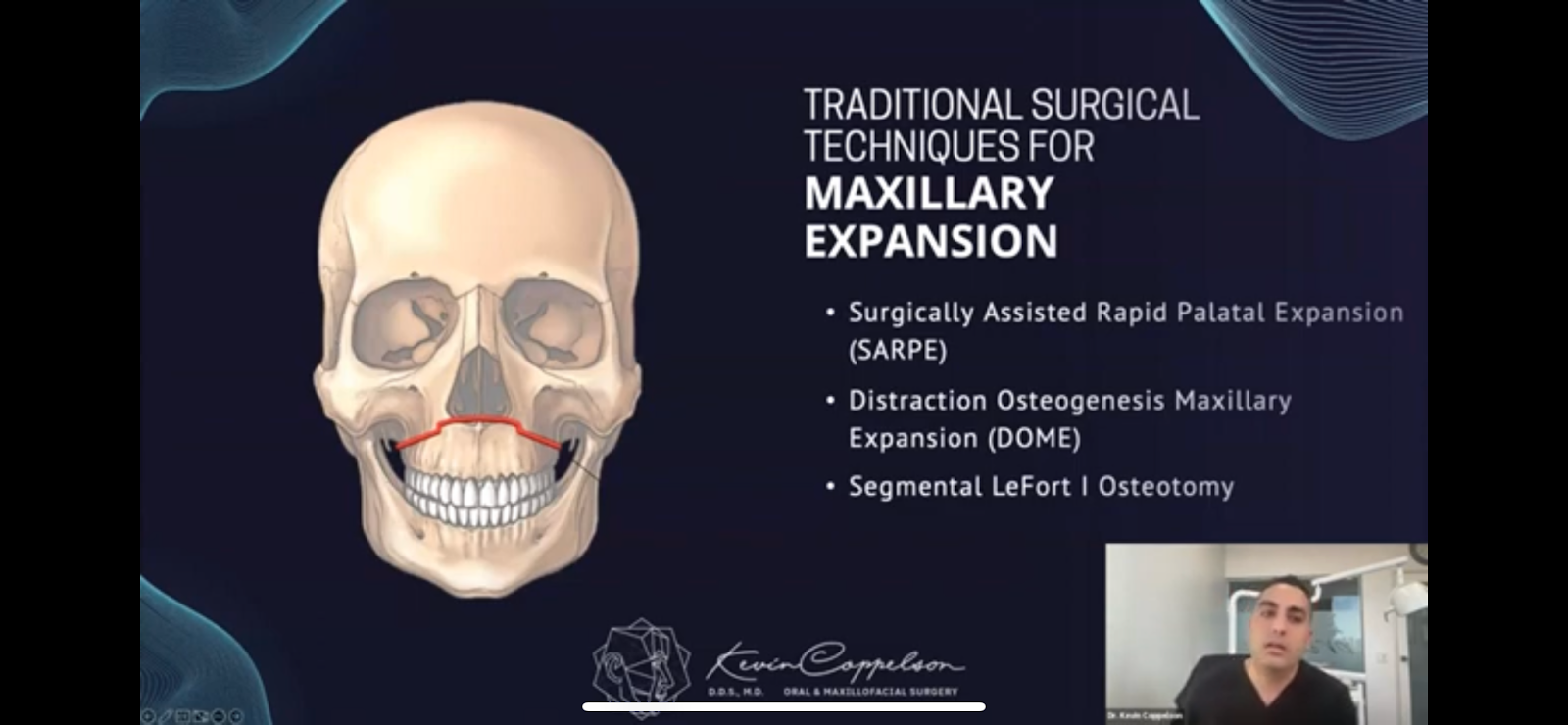
However, the problem with MSE that combines the Lefort 1 cut is that expansion will not enlarge the nasal cavity, it will simply enlarge the dental arches to create a wider smile and more tongue space. To increase the width and therefore volume of the nasal cavity, there should be only a cut of the palatal suture, no Lefort 1 cut - this procedure is referred to as MARPE, and it is the one we suggest.
This decision tree shows a comprehensive overview of all the available types of expansion. It is explained in more detail in the video, but below is a short explanation of each procedure for your reference

Dentoalveolar: related to the alveolar bone in which rooted the teeth
SFOT: grafting bone in front of the root of the teeth to allow more teeth movement during
orthodontic treatment.
Orthodontic expanders: various types of usually acrylic expanders to widen the dental arches. It
might also widen the maxilla and therefore the nasal cavity in children. For this, see the work of
the “Orthotropics” community comprised of orthodontists like Dr Mike Mew and Dr Simon Wong.
Skeletal/Basal Bone: the bone most of the maxilla is composed of, that is not in contact with the teeth.
Traditional: related to the traditional methods of expanding the maxilla with a Lefort 1 cut.
Miniscrew-Assisted Rapid Palatal Expansion (MARPE): maxillary expansion with a prior cut
of the palatal suture. These are the procedures that we think are better.
Simple MARPE: MSE with a cut of the suture through the mouth
Corticopuncture: multiple holes in the suture to facilitate the split (risks of failure to split).
EASE: a cut of the suture through the nose or mouth. Created by Dr Kasey Lee.
MIND: a cut of the suture above the teeth as shown in the photo above. Created by Dr
Coppelson.
In adults, MARPE is usually performed by a maxillofacial surgeon in conjunction with an orthodontist because it requires the surgical cutting of the maxillary suture, although some orthodontists perform the cut themselves under local anesthesia. This procedure is certainly more expensive than any other ENT intervention because it usually requires an orthodontic treatment (although not always). However, it can be partially or totally covered by insurance if you have sleep apnea or severe nasal obstruction which are often correlated. Unfortunately, many doctors are not aware of this procedure or think it’s too invasive and will prescribe classic ENT procedures as a first line of treatment. MSE is indeed a heavy treatment, but if you have the time and resources, we as ENS patients think that it is better to do MSE before any ENT procedure on your nose. If your nasal cavity has been properly expanded, you should not need turbinate reduction.
We hope this article has shed light on these practices and help you make the right decision for your health. Breathing is our most basic function, and everything else depends on it.
This article is co-written by Alexander CHALZ and Aurélien RUMIANO.
Main illustration by JawHacks, YouTube channel.